

Background: Reduced-intensity induction (RII) with imatinib yields comparable outcomes to HyperCVAD with imatinib with fewer induction deaths and an improved CR rate in Ph+ ALL (Chalandon. Blood. 2015). Dasatinib with steroids also produces excellent responses with little toxicity (Foa. Blood. 2011). Allogeneic bone marrow transplant (AlloBMT) remains the goal of therapy in Ph+ ALL based on contemporary trials with TKIs demonstrating improved survival in patients transplanted in CR1, and we have shown that transplant following induction with dasatinib yields better outcomes than with imatinib. Thus we implemented RII with dasatinib for the treatment of Ph+ ALL and compared to patients who received HyperCVAD with a 2nd generation TKI.
Methods: Patients with newly diagnosed Ph+ ALL admitted to Johns Hopkins Hospital from September 2017-June 2020 underwent a 4-week RII with: vincristine 2 mg/d weekly, dexamethasone 40 mg PO weekly on days 1 and 2, and dasatinib 100 mg PO daily. CNS prophylaxis with IT MTX was given on day 8. Dexamethasone and vincristine were reduced by 50% for patients over age 70. Filgrastim was started on day 15 for patients without ANC recovery. Patients who received HyperCVAD with dose adjustments for age (Rausch et al. Cancer. 2020) from July 2011-June 2020 were included for comparison. Dasatinib 100 mg PO daily or nilotinib 400 mg PO BID were given with HyperCVAD at the discretion of the treating physician. Rituximab 375 mg/m^2 on days 1 and 8 was given based on CD20 status. Subsequent therapy after induction was not specifically mandated.
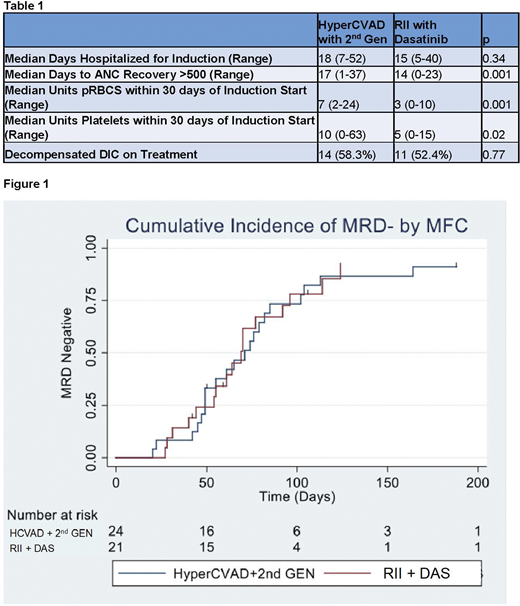
Results: 21 patients received RII and 24 received HyperCVAD. The cohorts were comparable in terms of gender (38.1% female vs. 50%, p=0.55), age (median 49.8 vs. 50.3, p=0.33), age >60 (33.3% vs. 29.2%, p>0.99), median WBC at diagnosis (19 vs. 23.5, p=0.56), and the presence of decompensated DIC (fibrinogen <150) prior to treatment initiation (4.8% vs. 8.3%, p>0.99). Among the patients treated with HyperCVAD, 15 received dasatinib (62.5%) and 9 received nilotinib (37.5%). Rituximab use was balanced between the cohorts (61.9% vs. 58.3%, p>0.99). Table 1 compares the time to ANC recovery >500, transfusion requirements within 30 days of chemotherapy initiation, rates of decompensated DIC following treatment initiation, and the duration of inpatient hospitalization for induction. While the rates of decompensated DIC were similar in each cohort, patients treated with RII required fewer platelet and pRBC transfusions. ANC recovery was faster following RII, and only 5 patients (23.8%) received growth factor support. All patients achieved a hematologic response. There was one induction death with HyperCVAD (4.2%). Most patients received a subsequent cycle of high-dose (HD) MTX and Ara-C with TKI (76.2% following RII and 91.7% following HyperCVAD). The remaining patients treated with RII subsequently received HD MTX (14.2%) or blinatumomab (9.5%) with TKI due to co-morbidities. Among those patients treated with HD MTX and Ara-C, blinatumomab was given with TKI to 6 patients (37.5%) who initially received RII and 1 patient (4.5%) after HyperCVAD (p=0.03) due to persistent MRD. As shown in Figure 1, the incidence of MRD-negativity by multi-color flow cytometry (MFC) with a sensitivity of 10-4 at day 120 after treatment initiation was similar for RII (85.4%, 95% CI 64.8-97.1) versus HyperCVAD (86.7%, 95% CI 69.8-96.6). Among patients subsequently treated with HD MTX and Ara-C, 62.5% proceeded to alloBMT after RII with an additional 12.5% currently undergoing transplant evaluation, while 86.4% proceeded to alloBMT after HyperCVAD. The 1-year RFS and OS following RII were 87.9% (95% CI 59.6-96.8) and 100% compared to 87.5% (95% CI 66.1-95.8) and 95.8% (95% CI 73.9-99.4) following HyperCVAD.
Conclusion: RII with dasatinib results in fewer transfusions and less myelosuppression compared to HyperCVAD with a 2nd generation TKI. More patients treated with RII received blinatumomab following high-dose MTX and Ara-C, but the rates of MRD-negativity were comparable between the two regimens. Thus RII with dasatinib followed by MRD-guided follow-up therapy facilitates MRD negative remissions with less toxicity than HyperCVAD. The vast majority of fit patients were able to proceed to alloBMT following either regimen. Transplant outcomes following dasatinib with induction are presented in our concurrent abstract demonstrating a 5-year RFS of 83% (95% CI 59.8-93.5).
Webster:Amgen: Consultancy; Pfizer: Consultancy. Jain:Bristol Myer Squibb: Other: for advisory board participation; CareDx: Other: Advisory Board; Takeda: Consultancy, Honoraria. Dalton:AbbVie: Research Funding; Eli Lilly: Research Funding. DeZern:Abbvie: Consultancy; Astex: Research Funding; Celgene: Consultancy, Honoraria; MEI: Consultancy. Gojo:Genentech: Research Funding; Amphivena: Research Funding; Merck: Research Funding; BMS: Membership on an entity's Board of Directors or advisory committees; Amgen: Research Funding. Bolanos-Meade:Incyte: Other: DSMB Fees. Luznik:WindMil Therapeutics: Patents & Royalties: Patent holder; AbbVie: Consultancy; Merck: Research Funding, Speakers Bureau; Genentech: Research Funding. Ali:Celgene: Membership on an entity's Board of Directors or advisory committees. Borrello:Celgene: Research Funding; Aduro: Patents & Royalties; WindMIL Therapeutics: Other: Founder , Research Funding. Wagner-Johnston:ADC Therapeutics, Regeneron, CALIB-R, Verastem: Membership on an entity's Board of Directors or advisory committees. Smith:Jazz: Consultancy, Membership on an entity's Board of Directors or advisory committees; Agios: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees. Levis:Menarini: Honoraria; Amgen: Honoraria; Daiichi-Sankyo: Honoraria; FujiFilm: Honoraria, Research Funding; Astellas: Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal